This is the second in a blog series on strategic planning in health care. The first piece described health care as an equation of great computational complexity with a variety of internal actors on one side reacting to large external social forces on the other. It focused on the value of adopting a scenario planning approach, allowing participants to “step back from their present quandaries and chart a strategic path with fresh eyes and a new perspective on future forces driving and shaping change.” In this piece we dig a little deeper into these forces and look at how distinctions among health care categories have changed, how they might continue to change, and consider some of the implications.
Looking at the evolution of health care over the last 30 years many of the boundaries that once characterized the system have become increasingly porous.
Categories that were once distinct have steadily blurred; health is not separate from social conditions; physical health and mental health are inextricably linked; care is not confined to clinical settings; care teams have expanded so apparent expertise is not confined to physicians— and all of this against the bigger “macro” story of the erosion of boundaries among medicine, business, technology, insurance, and consumer services.
Although many of these changes create challenges for all health care participants – patients, providers and institutions – not all of them are negative. The most profound blurring may have been the more widespread recognition of the social determinants of health; that many of the country’s largest health problems are not primarily medical.
A long list would include obesity, loneliness, gun violence, substance abuse, environmental exposure and health inequities. These arise from education, economics, culture, housing, working conditions, transportation, and politics as much as from biology. It is not hard to imagine medicine becoming increasingly involved in domains that previous generations would not have considered medical at all. The physician of 2050 may spend less time deciding which drug to prescribe and more time helping orchestrate a network of technological, behavioral, social, and community interventions.
We have seen the rise of “Dr. Google”– patients arriving with online research, or with digital monitoring data, and more recently with summaries from one of a number of AI ‘‘Doctors”, or sometimes not interacting with provider systems at all, preferring reliance on recommendations from AI, social media influencers and peer communities. Similarly the line between patient and consumer is already blurring dramatically, as many people continuously manage sleep, diet, metabolic health, cognitive performance and even longevity through systems that combine clinical and consumer services. Hospitals reinforce this by regularly surveying patients using questionnaires focused on consumer services & consumer-like attitudes.
This blurring will present a significant challenge for medical professionalism. The challenge is to preserve trust, accountability, and human judgment as the physician becomes just one actor within a much larger health ecosystem and their monopoly on information continues to erode.
Forces for Change Pushing in All Directions
We have mentioned quite a lot of categories and how they’ve been blurring, but this is not the only mechanism making strategic planning in health care so challenging, as of course none of these are static phenomena. They interact and affect each other and are affected by larger forces for change, which can be disruptors as well as accelerants.
This is particularly true in health care systems, structures and economics. The steady rise in spending, and the belief that more spending would naturally lead to better outcomes, has given way to a growing focus on value, outcomes, waste reduction, and affordability.
Looming large over all of this is government involvement. Medicare and Medicaid account for a substantial and growing share of federal spending as life expectancy increases and boomers age (See table below).
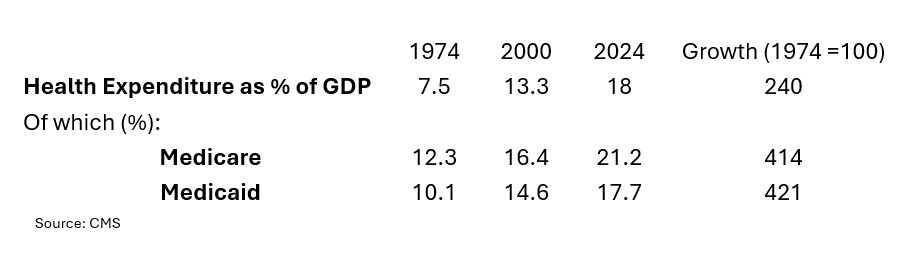
Long-term fiscal pressures will act as a kind of forcing function on US government support for Medicare, Medicaid and veterans’ health benefits. (Just taking the Medicare example, the Hospital Insurance Trust Fund (Part A) is projected to run out by 2033.) To maintain these programs at current levels will require some (politically tricky) combination of increased taxes, reduced benefits, higher eligibility ages, stronger cost controls and, perhaps most of all, productivity improvements.
Aggregating all these dynamics leads to just more questions and uncertainty in the health care domain.
One can make a plausible case for extreme fragmentation of delivery systems as easily as one can for accelerated consolidation. Taken to an extreme, this blurriness combined with spreading dissatisfaction with the quality of care and services could provoke a regulatory counter-revolution with stricter controls and tighter boundaries.
Clearly, there is no credible “most likely case” for US health care that strategists can plan on.
Creating a Sharper Strategic Focus
For the last dozen years, FSG has been involved in strategic planning in health care, successfully applying scenario planning to help accrediting bodies, specialty boards, medical and nursing schools, and professional organizations make prudent investments and manage strategic risks. The diversity of our scenario workshop teams – from medical residents to hospital CEOs and all stakeholders in-between – make our workshop discussions uniquely rich and productive.
Scenario planning is always about imagination and rigorous thinking and collaborative deliberation around strategic options. With health care being buffeted by technological change, new players, and extreme financial challenges it seems that the scenario approach is the only way to get out ahead of the changes and see past the fog that obscures the path forward.
While you make the good point that the blurriness in health care has positive as well as negative qualities I see great challenges ahead for regulators and medical gatekeepers as they try to uphold clear and meaningful standards of patient care and even what it means to be a physician.
Agree. But I wonder what process would be necessary to keep these standards clearly defined in a way that also recognizes the way the world has changed and continues to change. I keep thinking that there are parallels with constitutional amendments and the argument between ‘originalists’ and those that feel amendments are overdue.
Shortly after I finished this piece I listened to an Economist podcast about edible technology – https://www.economist.com/podcasts/2026/06/10/eat-your-electronics-boost-your-health – that is, devices that are made from food, as opposed to things that can be ingested, like small cameras which have been around for a while. It is hoped that in a few years we could have autonomous edible devices that can detect, for instance a polyp, evaluate and make a decision that the polyp is the size that needs a volume or particular concentration of a payload or a drug, and deliver it. This would certainly be boundary blurring.
But what particularly struck me was an engineer’s evaluation of the work he is doing – “I also want to emphasize the fact that the beauty of this field is, in my opinion, that it’s truly interdisciplinary. Because it’s not only engineers like me who develop the technologies and would do the systems integrations, particularly of these components. We need to work with material scientists. We need to work with computational data analytic experts. We have to work with epidemiologists. We need to understand how society would be willing to use these devices. We all have to to work together and not to mention the medical doctors. I mean, they must be with us from the beginning to the end.”
And “how society would be willing to use these devices” might be the most important and challenging link in the chain of roles and activities you describe, given the resistance in 2026 to vaccines in some segments of society.
Boundary blurring is a phenomenon we find in nearly every scenario-planning project I have ever been part of.
It is a characteristic of our age that all kinds of industries find themselves contending with new entrants from directions they never previously considered. Radio, banking, shipping, Hollywood, telephone, retailing….
Without even realizing that they are doing it, every established industry resists imagining that the players in their ecosystem will ever change. Player characteristics may alter, of course. but the faces will be familiar.
The first deliverable of scenario planning, I would argue, is getting clients to imagine a world of unfamiliar faces.
You are right Kevin. And it is easier to imagine a world of unfamiliar faces when you are having to react, with your scenario planning workshop teammates to conditions in an unfamiliar world.
Kevin McDermott is right about how often we have witnessed this blurring of boundaries phenomenon in scenario planning. I went back to my first scenario project in 1984 for USAF XOXIP to have a look for boundary blurring. While we did not call it that, we did identify numerous future threats with that characteristic.
However, the point I would emphasize is that this phenomenon should not be viewed only as a threat or a disturbance in the force. It is simply a strategic tendency we have seen – although a pretty interesting one.
An automotive client in the mid 1990s asked us (during a second scenario planning project) to investigate how stable the emerging SUV trend (a blurring, for certain) was likely to be. It turned out to be quite robust. However, that company did not rush to alter its vehicle mix. Instead it waiting for the market to settle while it planned for category expansion, it thought carefully about sedan viability, and it looked hard at potential sub-systems compatibilities.
They saw threat and opportunity and chose opportunity solidly based around some company core competencies. I would argue the House of Medicine must do the same. I would further argue that the core competency they must use to plan for and mange the blurring is the experience, skills, and professionalism of MDs and DOs.